
Is Ketamine an Opioid? Why One of These Painkillers is Safer Than the Other
Last reviewed and updated: May 11, 2026.
The short answer: no — ketamine is not an opioid. They are different drug classes acting on different receptors, with very different addiction profiles.
Ketamine and opioids are both used for pain, both are controlled substances, and both can cause dissociative or sedating effects at sufficient doses. That’s where the similarity ends. They are entirely different drug classes, acting on entirely different receptor systems, with entirely different risk profiles.
This guide explains the actual difference and why ketamine is increasingly used as an alternative to opioids — especially for chronic neuropathic pain. Pricing data is drawn from our verified pricing across 1,800 clinics across 1,800 verified U.S. ketamine clinics, October 2022 through March 2026.
Key Takeaways
Five clean differences — drug class, schedule, addiction signal, pain type, and cost — separate the two.
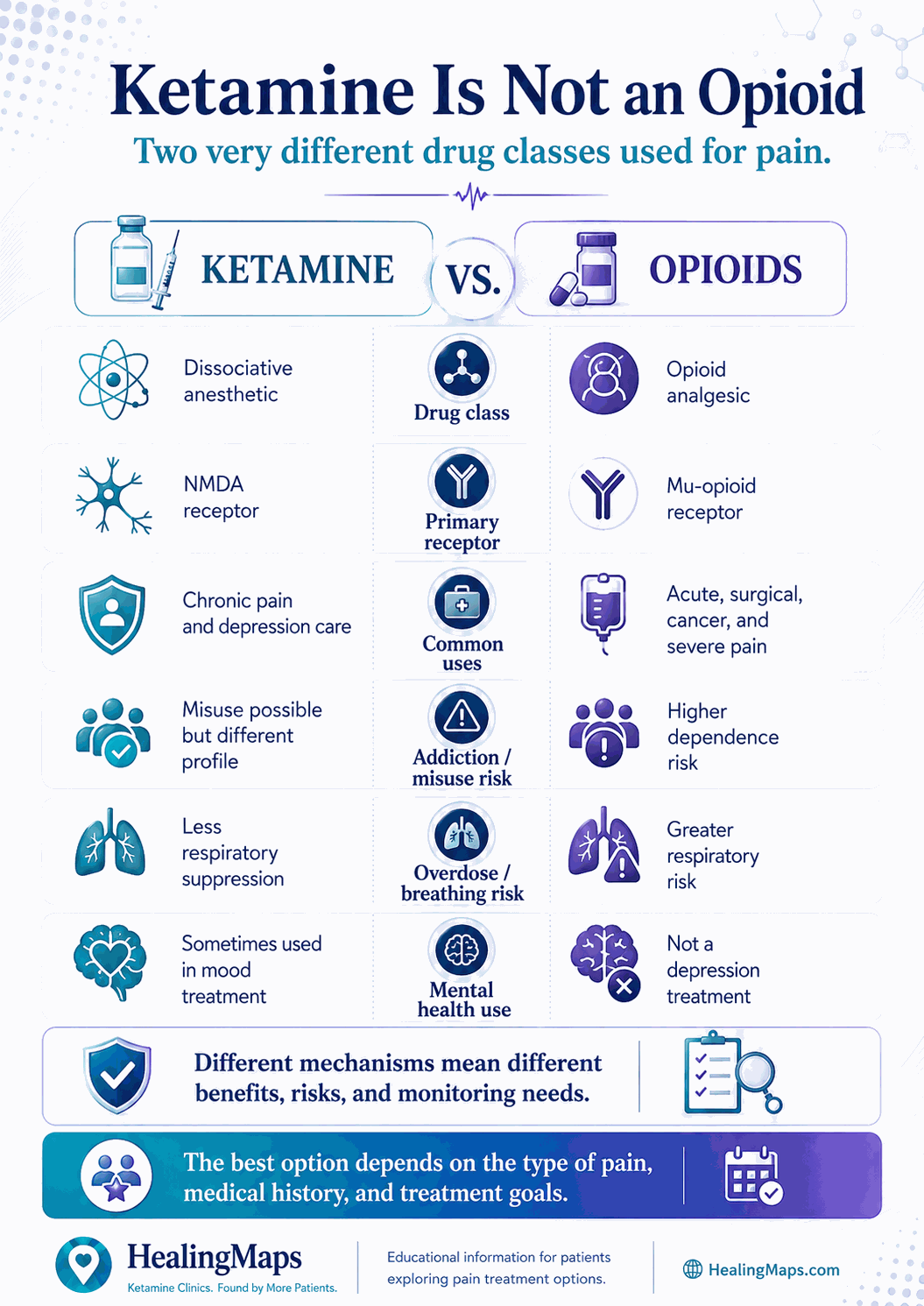
| Different drug classes | Ketamine = NMDA antagonist. Opioids = mu-opioid receptor agonists. Entirely different pharmacology. |
| Different DEA schedules | Ketamine = Schedule III. Most prescription opioids = Schedule II. Different abuse-potential category. |
| Different addiction risk | Therapeutic ketamine carries a low addiction signal. Opioids drive ~80,000 U.S. overdose deaths annually. |
| Different pain types | Ketamine works for neuropathic and central pain. Opioids work for acute nociceptive pain. |
| Different cost profiles | Ketamine = $300–500 per session in-clinic. Opioids = $5–50 per month for generics. |
Visualized side-by-side, ketamine and opioids share almost nothing except the job they do.
The Pharmacology: Why They’re Not the Same
Opioids work by binding to the mu-opioid receptor in the central nervous system. This dampens pain signaling and produces euphoria, sedation, and respiratory depression. The same mechanism that relieves pain is also responsible for opioid-related overdose deaths — at high enough doses, opioids suppress breathing.
Ketamine works by blocking the N-methyl-D-aspartate (NMDA) receptor, which is part of the glutamate signaling system in the brain. This produces dissociation, analgesia, and (at therapeutic doses) rapid antidepressant effects. The NMDA pathway is a different family from the mu-opioid pathway, and ketamine does not produce significant respiratory depression at therapeutic doses.
This is why ketamine appears on the WHO List of Essential Medicines and is the anesthetic of choice in trauma medicine, conflict zones, and pediatric emergency departments — it preserves cardiovascular and respiratory function more reliably than opioid-based anesthesia.
Why the Confusion?
Patients sometimes assume ketamine is an opioid because of overlapping use cases (pain management) and overlapping vocabulary (“dissociation” is sometimes mistaken for “sedation”). The DEA also classifies both as controlled substances, which signals “addictive drug” to many people regardless of the underlying pharmacology.
The actual classification is informative. Ketamine is DEA Schedule III — the same category as anabolic steroids and ketamine analogs — meaning it has accepted medical use and a lower potential for abuse than Schedule II substances. Most prescription opioids (oxycodone, hydromorphone, fentanyl, morphine) are Schedule II, the highest category for substances with accepted medical use. Heroin is Schedule I, meaning the DEA does not recognize accepted medical use.
Addiction Risk: A Real Difference
The opioid crisis is among the largest public health emergencies in the United States. CDC data show roughly 80,000 annual overdose deaths involving opioids in recent years. The addictive potential of opioids — especially synthetic opioids like fentanyl — is well documented.
Ketamine has a different risk profile. At therapeutic doses (4–6 IV/IM sessions in a clinical setting, or sublingual lozenges at prescribed doses), addiction events are rare. The pattern of clinical use — bounded dosing, no patient-controlled escalation, integration with therapy — is designed to keep abuse potential low.
Recreational use is a different matter. Heavy daily ketamine use (“K-holing” multiple times per week) can produce psychological dependence and a documented condition called ketamine cystitis (severe bladder inflammation). These are real risks, but they are tied to the unsupervised abuse pattern, not the clinical pattern.
Pain Management: Where Each Wins
Where opioids work better
Acute nociceptive pain — post-surgical, fracture, cancer pain, severe injury. Opioids remain a standard of care for these indications, with the caveat that prescribers now favor short courses to reduce dependence risk.
Where ketamine works better
Chronic neuropathic and central pain — complex regional pain syndrome (CRPS), fibromyalgia, post-herpetic neuralgia, refractory migraine and cluster headaches. These pain syndromes often do not respond to opioids and may even worsen on long-term opioid therapy (a phenomenon called opioid-induced hyperalgesia).
Ketamine’s NMDA-antagonist mechanism appears to interrupt the central sensitization that drives chronic pain, where opioids merely dampen the signal at the receptor level. For patients who have been on long-term opioids without adequate relief, ketamine is increasingly being used as an opioid-sparing or opioid-replacing intervention.
Cost: Not a Fair Comparison
Generic oral opioids cost $5–50 per month. Ketamine in-clinic costs $300–500 per session, with most pain protocols requiring 4–6 sessions of induction plus periodic maintenance. The dollar gap is large, but it does not reflect total cost of care — long-term opioid use carries dependence, tolerance, hyperalgesia, and overdose risk that creates downstream cost (substance use disorder treatment, lost work, hospitalizations).
For patients with chronic neuropathic pain who have not responded to opioids, the relevant comparison is not “ketamine vs. opioids per session” but “ketamine therapy vs. years of unrelieved chronic pain.” That changes the calculation.
Frequently Asked Questions
Is ketamine an opioid?
No. Ketamine is an NMDA receptor antagonist. Opioids are mu-opioid receptor agonists. They are different drug classes with different mechanisms of action.
Is ketamine safer than opioids?
For chronic neuropathic pain, generally yes — ketamine carries a meaningfully lower addiction risk and does not cause respiratory depression at therapeutic doses. For acute post-surgical pain, opioids remain a standard of care because of their reliable, fast-acting analgesia.
Can ketamine replace my opioid prescription?
Sometimes. For chronic neuropathic pain, many patients successfully transition from long-term opioids to ketamine therapy plus adjunct treatments. This should be done under the care of a pain specialist who can manage the taper.
Can I take ketamine and opioids together?
Combinations are sometimes used clinically (especially in inpatient and post-surgical settings), but only under direct medical supervision. The combination changes the risk profile of both drugs and should never be self-managed.
The Bottom Line
Ketamine is not an opioid. They are different drug classes, on different receptors, with different addiction profiles, treating different kinds of pain. For chronic neuropathic pain that has not responded to opioids — or where opioid use carries unacceptable risk — ketamine is increasingly being used as an alternative.
Find a verified ketamine clinic near you: Browse 1,800 mapped ketamine clinics across all 50 states.
READ NEXT: Ketamine Infusion Cost: Price Ranges for Depression, Pain and Other Treatments

