
Why Timing Matters: The Science Behind Scheduling Psychotherapy After Ketamine
Ketamine practitioners face a critical question when integrating psychotherapy into treatment protocols. Should therapy happen during the ketamine session, immediately after, or the following day? New insights from Yale researcher Dr. Samuel Wilkinson suggest the answer lies in understanding how ketamine reshapes the brain. Read the full interview Dr. Wilkinson on Psychedelic Alpha here.
Do you work in the ketamine industry? Save thousands on overhead, medmal insurance, and other fees by joining the first GPO for ketamine clinics and practitioners. There’s no cost to join and zero obligations. Sign up here!
Key Takeaways
| Factor | Clinical Implication |
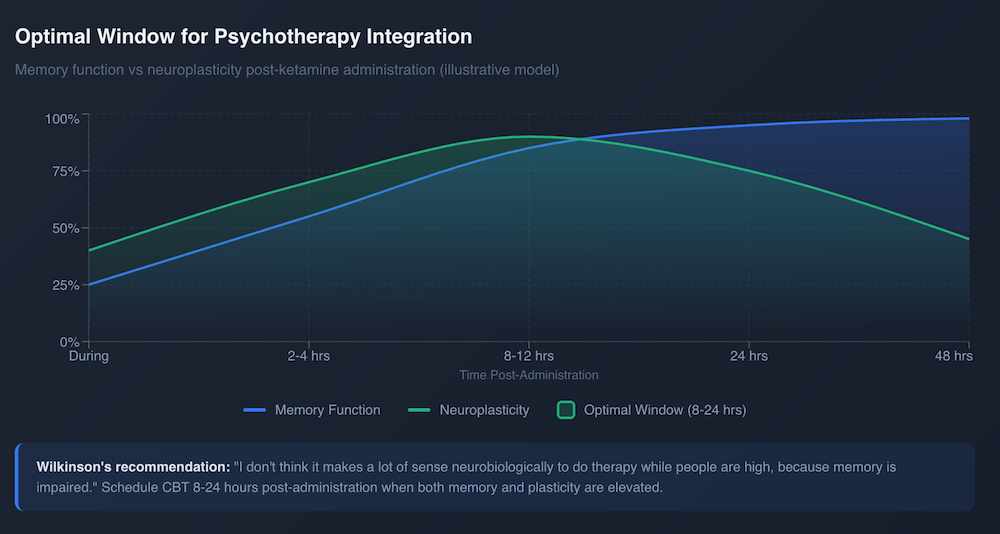
| Optimal Window | Schedule psychotherapy 8 to 24 hours after ketamine administration |
| During Session | Memory impairment makes therapy less effective while patients are dissociated |
| Plasticity Peak | Neuroplasticity peaks at 24 to 72 hours, creating ideal conditions for cognitive restructuring |
| Evidence Base | CBT delivered post ketamine extended remission to eight weeks in Yale studies |
| Key Caveat | Benefits appear limited to patients who first respond to ketamine itself |
Looking for treatment? Find ketamine clinics closest to you as well as other psychedelic therapies in your area.
The Neurobiology Argument
In a recent interview with Psychedelic Alpha, Wilkinson was direct about the timing question. He noted that conducting therapy while patients are dissociated does not make neurobiological sense. Memory is impaired during the acute phase. Patients struggle to encode new information when ketamine is actively affecting their brain.
The science supports his view. Research published in Biological Psychiatry found that ketamine’s plasticity potential increases significantly within two hours of administration. This elevated state persists for several hours. However, the structural changes that support lasting improvement happen later. Dendritic spine formation peaks between 24 and 72 hours after treatment.
This creates a window. The brain becomes more receptive to change. New neural connections form more readily. Thought patterns become more malleable. Wilkinson’s studies at Yale delivered cognitive behavioral therapy 8 to 24 hours after ketamine infusions. The goal was to catch patients when memory function had recovered but neuroplasticity remained elevated.
What the Clinical Data Shows
Wilkinson’s randomized trial found that CBT following ketamine produced a moderate to large effect size for sustaining antidepressant benefits. Responders who received therapy maintained remission for up to eight weeks after their last infusion. The relapse rate dropped to 25 percent at the end of the CBT course.
One important caveat emerged. Patients who did not respond to ketamine initially showed no benefit from adding therapy. The plasticity window appears to require a biological response to ketamine before psychological interventions can build upon it.
Practical Implications for Clinics
Wilkinson acknowledged that some practitioners conduct therapy during monitoring out of convenience. Someone has to watch the patient anyway, so why not use that time productively? The answer is that timing affects outcomes. The evidence suggests waiting.
For practitioners designing protocols, consider scheduling therapy appointments for the day after ketamine sessions. This approach captures the neuroplasticity window while ensuring patients can fully engage in the therapeutic process. It may also reduce the need for indefinite maintenance dosing.
The research remains preliminary. Wilkinson himself called the evidence for psychotherapy improving outcomes beyond ketamine alone low level. Larger trials are underway. But the neurobiological rationale is sound. The brain is most ready to change after the drug has cleared but before the plasticity window closes.
Practitioners who align their protocols with this biology may find their patients achieve more durable results.

