
What the FDA’s New Psychedelic Rulebook Means for Ketamine Clinics
On July 13, 2026, the FDA finalized its first formal guidance for studying psychedelic drugs in people. The rules cover psilocybin, LSD, and MDMA. They do not cover ketamine. So a ketamine clinic owner could skim the headlines and move on. That would be a mistake. This guidance is the clearest signal yet that a new category of treatment is about to arrive, and ketamine clinics are the infrastructure best positioned to deliver it. Here is what the moment actually means for your practice. The enforcement side arrived the same month, when the FDA targeted online ketamine sellers.
Do you work in the ketamine industry? Save thousands on overhead like medical supplies, professional insurance and more by joining the first GPO for ketamine clinics and practitioners. There’s no cost to join and zero obligations. Sign up here!
Key Takeaways
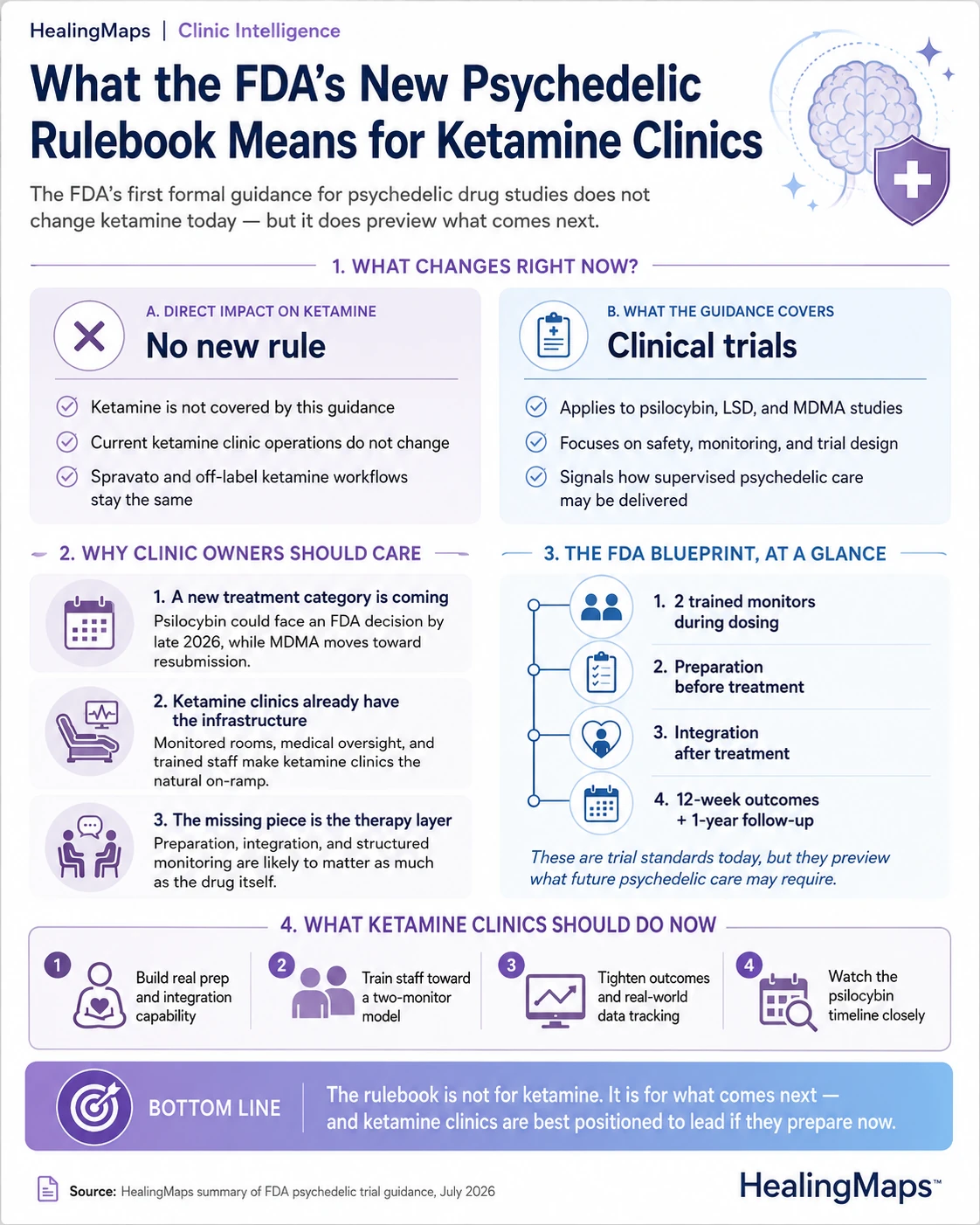
| The guidance covers trials, not ketamine | The FDA’s new rules govern clinical trials for psilocybin, LSD, and MDMA. They do not change how ketamine clinics operate today. |
| Ketamine is not affected directly | Ketamine is an approved medication and is not a Schedule I psychedelic, so the guidance adds no new rule to your current practice. |
| The real signal is timing | Psilocybin could reach an FDA decision by late 2026, with MDMA working toward resubmission. A new treatment category is arriving. |
| Ketamine clinics are the on-ramp | Supervised dosing, medical oversight, and trained staff make ketamine clinics the natural home for future psychedelic care. |
| Build the therapy layer now | The guidance’s preparation, integration, and monitoring standards preview what psychedelic therapy will require. |
First, What This Does Not Change
Start with the reassurance. Ketamine is not a Schedule I drug. It is an approved anesthetic used off label for depression, and Spravato is FDA approved for treatment-resistant depression. The new guidance governs clinical trials for Schedule I psychedelics. It does not touch how you run ketamine treatment today. Your protocols, your prescribing, and your daily practice are unaffected. Nothing in this document adds a rule to your current work.
Why Ketamine Clinics Should Read It Anyway
Now the part that matters. The FDA paired this guidance with priority review vouchers for psilocybin developers, including Compass Pathways and the Usona Institute. Those vouchers can compress review from about a year to one or two months. A decision on psilocybin for depression could land by late 2026. MDMA is being redesigned for resubmission after its 2024 rejection. The whole category is moving toward approval. When these therapies clear the FDA, someone has to deliver them in a clinical setting. Ketamine clinics already have the rooms, the monitoring, and the medical oversight.
The Blueprint Is in the Safety Section
Read the guidance’s safety requirements as a preview of what psychedelic therapy will demand. Two trained monitors watch each dosing session. Patients get preparation before and integration after. Sponsors must measure the effect at 12 weeks and follow patients for a year. Much of this will feel familiar, because you already run monitored dosing sessions. The gap for most ketamine clinics is the psychological layer, the preparation and integration work that turns a drug session into a course of therapy. Clinics that build that capability now will not have to scramble later.
The VA Just Pointed the Way
On the same day, the VA and HHS signed a five-year partnership to prepare the veterans health system for FDA-approved psychedelic treatments. A second agreement links the VA and the FDA directly on data and evidence. The details matter less than the signal. The federal government is now building the clinical infrastructure to deliver supervised, medically overseen psychedelic care at scale. That is the same model ketamine clinics already run, and the VA has used ketamine and Spravato for veterans with depression for years. The direction of travel is clear.
The Head Start Is Real
Here is the strategic point. Ketamine is the only widely available option in this category right now. That gives established clinics a head start that is hard to buy later. You have referral relationships, trained staff, monitored space, and patients who already trust the setting. HealingMaps has tracked more than 23,496 patient inquiries across 1,800 verified clinics, which is a demand base that is already looking for supervised care. When psilocybin and MDMA arrive, the clinics positioned to add them will be the ones that already deliver medically overseen treatment. That is you.
What to Do Now
A few concrete moves separate the clinics that will lead from the clinics that will follow. The first is building real preparation and integration capability, since that psychological layer is where psychedelic therapy lives. The second is training your staff toward the two-monitor model the guidance describes, because that standard will likely carry into approved psychedelic care. The third is getting your outcomes data in order, since real-world evidence is becoming currency with both regulators and payers. The fourth is tracking the psilocybin timeline closely, because the clinics that plan around a late 2026 decision will move first.
What It Means for the Road Ahead
This guidance marks the moment psychedelic medicine stopped being a curiosity and became a category in development. Ketamine clinics sit at the front of that category. Not because ketamine is a classic psychedelic, but because you already do the hard part, which is delivering a mind-altering treatment safely under medical supervision. The rulebook the FDA just wrote is for the therapies coming next. The clinics that read it as their own on-ramp will shape the next phase of this field.

