
How To Start Microdosing Psychedelics: A Beginner’s Guide
Last reviewed and updated: May 11, 2026.
Microdosing remains illegal under U.S. federal law except in Oregon and Colorado. This guide is informational, not a recommendation to break the law.
Microdosing — taking sub-perceptual doses of a psychedelic on a structured schedule — has become a topic of mainstream interest. Tech workers, creative professionals, and people managing mood symptoms have all reported using it. The research is more cautious than the popular narrative; recent placebo-controlled studies suggest a meaningful share of self-reported benefit comes from expectancy effects.
This guide compares the three best-known microdosing protocols, summarizes what the controlled research actually shows, and is direct about the legal and safety considerations. It is not a how-to for breaking federal law.
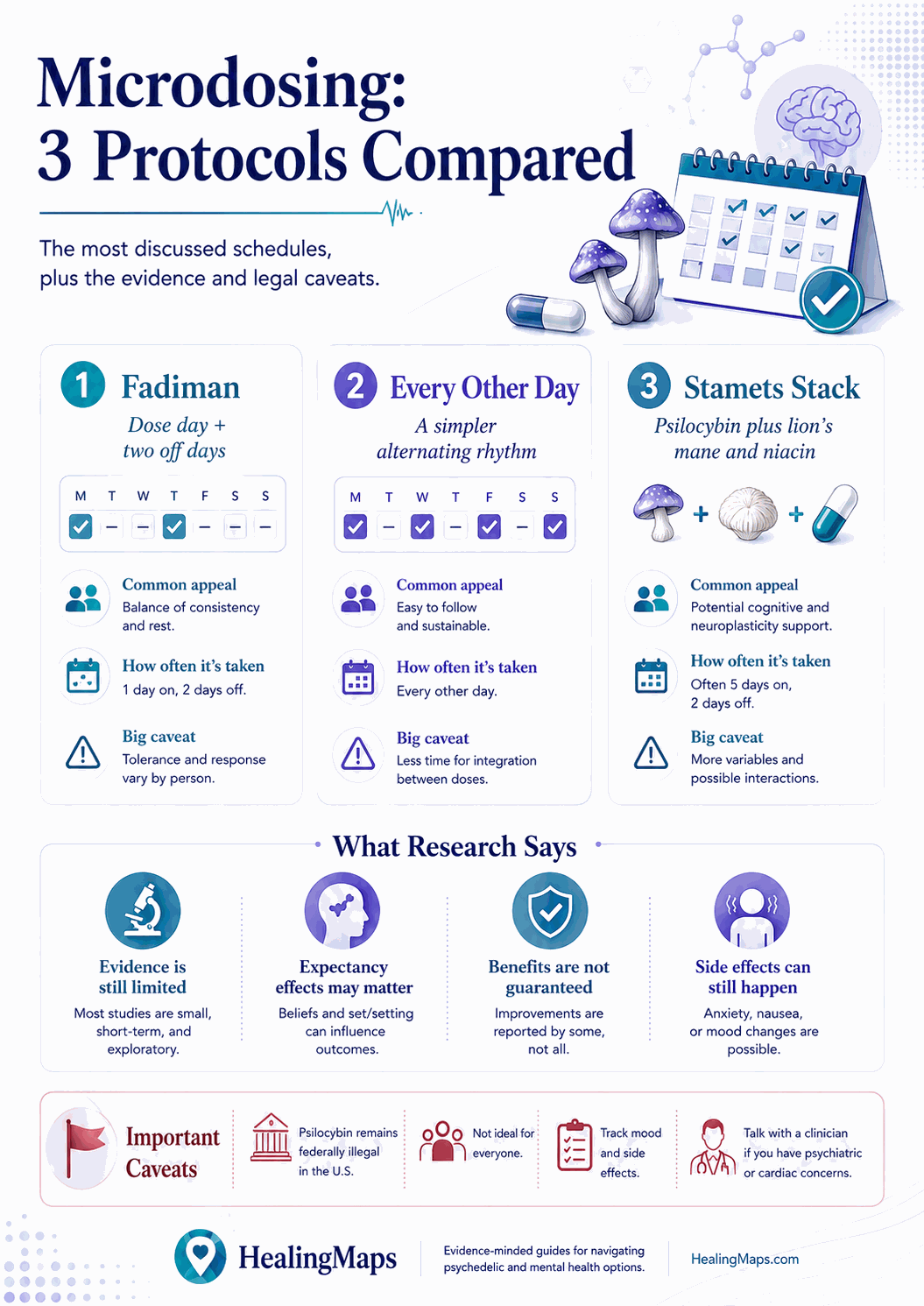
Three protocols dominate the published microdosing literature. Each handles tolerance and dose schedule differently.
What Microdosing Means
A microdose is a sub-perceptual dose of a psychedelic — typically one-tenth to one-twentieth of a recreational dose. The goal is no acute psychedelic effect: no visual changes, no ego dissolution, no “trip.” The dose is meant to nudge mood, focus, or creativity without disrupting normal function.
Most discussions center on psilocybin (in dried mushroom form) and LSD. Other compounds — DMT, mescaline, ibogaine — are sometimes microdosed but with less established protocols and a thinner safety base.
The Three Best-Known Protocols
The Fadiman Protocol
Developed by James Fadiman, a psychologist and longtime psychedelic researcher. The schedule is one day on, two days off — dose Day 1, rest Days 2–3, dose Day 4, repeat. The two rest days are designed to clear acute tolerance, which builds quickly with daily psychedelic dosing.
Typical dose for psilocybin: 0.1–0.3 grams of dried mushrooms. The protocol is run for 4–8 weeks, followed by a 2-week break before any subsequent cycle. Most published microdosing self-report studies use this protocol.
The Stamets Stack
Developed by mycologist Paul Stamets. The schedule is four days on, three days off. The full stack pairs the psilocybin microdose with 50–200 mg of lion’s mane mushroom and 100–200 mg of niacin (vitamin B3). The hypothesis is that this combination promotes neurogenesis and synaptic plasticity beyond what psilocybin alone produces.
The Stamets stack has compelling theoretical underpinnings but limited controlled-trial evidence on the specific combination. Most users adopt it for the neuroplasticity hypothesis rather than for documented superiority over the Fadiman schedule.
The Nightcap or Random Protocol
Less of a formal protocol, more a usage pattern. Dose only when a specific context calls for it — a creative work session, a brainstorming meeting, a social event where social anxiety would otherwise dominate. There is no fixed cadence; tolerance management depends on user self-awareness.
Popular in tech and creative communities. Minimal published research on this specific pattern. Higher risk of tolerance buildup if used too often without explicit rest periods.
What the Research Actually Shows
Microdosing self-reports are overwhelmingly positive. Survey-based research (often referencing Fadiman protocol users) consistently shows reported improvements in mood, focus, creativity, and social ease. These studies use observational methods — participants know they are microdosing, expect benefit, and self-report.
Placebo-controlled studies tell a more complicated story. The most-cited is Szigeti et al. (2021), a self-blinded study where participants did not know whether they were taking microdoses or placebos. Both groups reported improvements; the placebo group’s improvements were not significantly different from the microdose group’s. The interpretation is that expectancy effects account for a substantial share of self-reported microdosing benefit.
This is not a refutation of microdosing — it is a recalibration. Some patients in some contexts may benefit from sub-perceptual psychedelic dosing in ways that go beyond placebo. The evidence does not yet support strong claims about it.
Legal Context
Psilocybin and LSD are Schedule I controlled substances under the U.S. federal Controlled Substances Act. Possession, distribution, and personal cultivation carry federal penalties.
Two states have created legal pathways for psilocybin specifically:
- Oregon — Measure 109 (2020) created a state-licensed psilocybin services program. Use is limited to licensed service centers under facilitator supervision; personal possession outside the program remains illegal.
- Colorado — Proposition 122 (2022) decriminalized personal use of psilocybin and is rolling out a regulated therapy program through 2026.
Several cities have separately decriminalized possession (Denver, Oakland, Santa Cruz, Seattle, Detroit), but decriminalization is not legalization — possession remains technically illegal under federal law and may still draw state charges depending on jurisdiction.
Safety Considerations
Sourcing. Unregulated supply means you may not know the actual potency or purity of what you are taking. Misidentified mushroom species can be toxic. Mass-produced “magic” chocolates and gummies have inconsistent dose distribution.
Drug interactions. Psilocybin and LSD interact with several medications, especially SSRIs and MAOIs. Concurrent use of lithium with psychedelics has been associated with seizures.
Mental health. Personal or family history of psychosis, schizophrenia, or bipolar disorder are contraindications. Microdosing can trigger or exacerbate psychotic symptoms.
Cardiovascular. LSD and psilocybin both have mild cardiovascular effects; uncontrolled hypertension or significant cardiac history are contraindications.
If You’re Curious About Psychedelic Therapy Generally
Patients interested in psychedelics for mood or trauma symptoms have several legal options that don’t involve federal-law violations:
- Ketamine therapy — legal nationwide, FDA-approved as Spravato for treatment-resistant depression. Find a verified clinic.
- Psilocybin in Oregon or Colorado — through licensed service centers, with facilitator supervision.
- MDMA-assisted therapy — currently in late-stage clinical trials. The FDA review is ongoing as of mid-2026; access today is largely through clinical trial enrollment.
- Clinical trials — psilocybin trials at Johns Hopkins, NYU, UCSF, and others recruit ongoing.
The Bottom Line
Microdosing is interesting and worth more research. It is also illegal under federal law in most contexts, comes with a legitimate placebo-effect question, and carries safety considerations that get glossed over in popular coverage.
If you’re drawn to psychedelics for mood or trauma symptoms, ketamine therapy is the closest thing to “psychedelic medicine” available legally and under clinical supervision in 2026. See our breakdown of at-home vs in-clinic ketamine for context on the most common entry point.
READ NEXT: Psychedelic Clinical Trials: Current Studies and How to Participate

