
At-Home Ketamine Treatment Vs In-Clinic Ketamine Experiences: Pros and Cons
Last reviewed and updated: May 11, 2026. Medically reviewed by Dr. Abid Nazeer, MD.
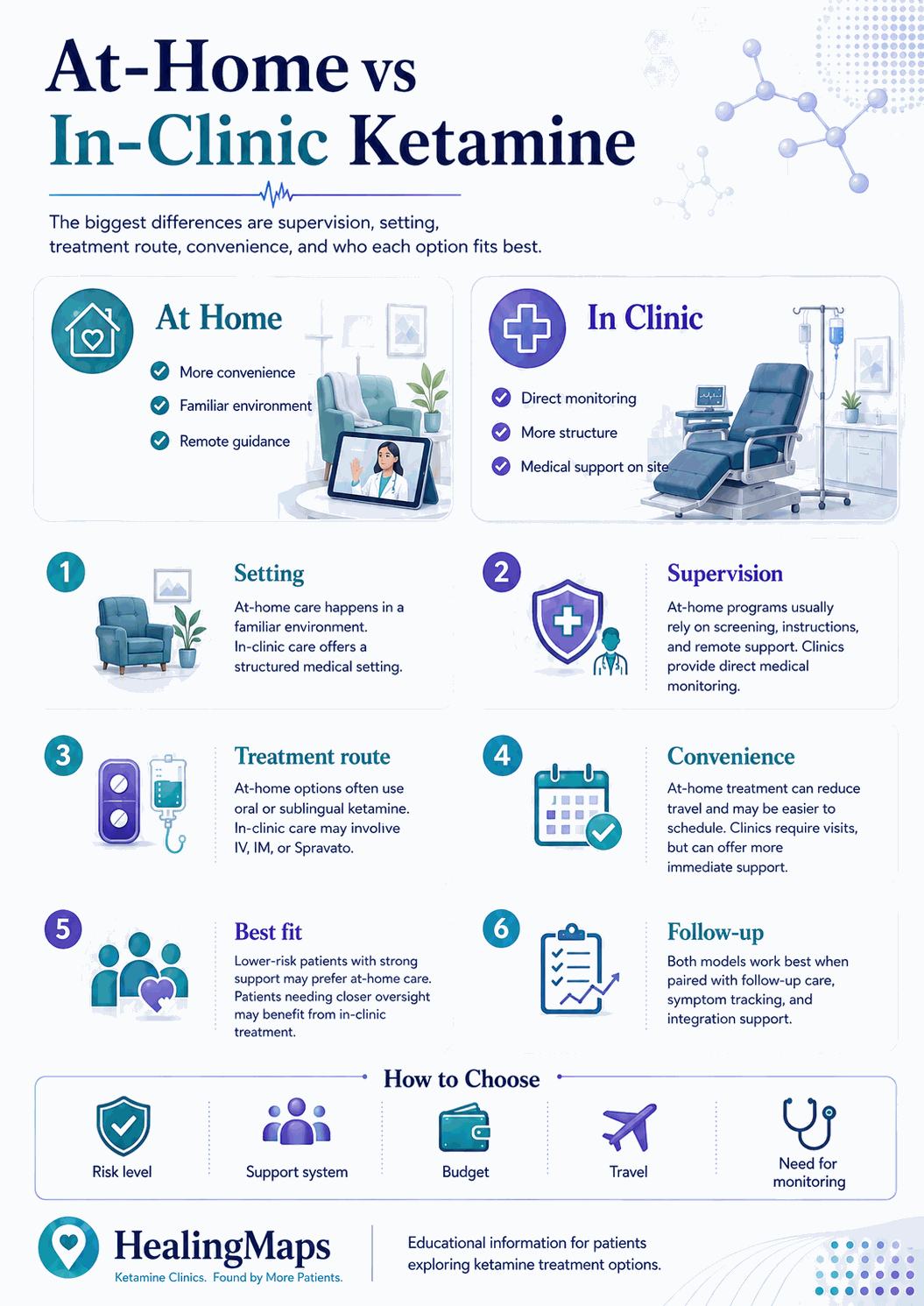
The choice between at-home ketamine and in-clinic ketamine is rarely a clean decision. Patients want the access and lower cost of telehealth. They also want the safety net of a clinical setting. Most decide based on hearsay or marketing, not data. The evidence base behind the at-home model is itself contested, as our review of the Mindbloom affiliated injection study shows.
This guide breaks down the decision using a different lens. We analyzed 23,496 patient inquiries collected across 1,800 verified U.S. ketamine clinics between October 2022 and March 2026. The dataset includes 658 practitioner survey points and a verified pricing across 1,800 clinics. Where most articles on this topic recycle generic pros and cons, we use the actual answers patients gave when they were trying to make this choice.
Key Takeaways
Below, the rest of the comparison — cost, insurance, schedule, hybrid models — at a glance.
| Cost gap | At-home runs $150–250/month for sublingual maintenance. In-clinic runs $300–500 per IV/IM session. Both rarely covered by insurance. |
| Insurance reality | 75% of inquiring patients have zero coverage in either setting. Spravato is the exception ($0–250 copay when prescribed in-clinic). |
| Safety perception | 64.8% of patients we surveyed flagged at-home ketamine as “a bad idea” on safety grounds. |
| Access reality | 58.1% say telehealth ketamine increases access. 44.9% cite access as their top barrier to treatment. |
| Hybrid is the new norm | Most clinics now combine in-clinic induction with at-home maintenance, capturing both safety and access advantages. |
Visualized side-by-side, the cost gap is smaller than telehealth marketing implies — and the safety/access tradeoff is the more decisive one.
The Cost Reality
Cost is the most cited reason patients consider at-home ketamine. The gap is real, but smaller than most marketing copy suggests once you factor in dose density and protocol length.
At-home (sublingual or rapid-dissolve tablets): $150–250 per month for maintenance. Subscriptions usually bundle the medication, asynchronous clinician check-ins, and a video onboarding session.
In-clinic (IV or IM): $300–500 per session is the national pricing sweet spot. Most patients complete a 6-session induction over two to three weeks. That puts the upfront cost at roughly $1,800–3,000 before maintenance begins.
Insurance does not change the math much. In our 23,496-inquiry dataset, 75% of patients had zero coverage for ketamine therapy in either setting. The published cash price is the price they will pay. Spravato (esketamine) is the one exception — when prescribed in-clinic, copays run $0–250 per session for insured patients.
RELATED: Ketamine Infusion Cost: Price Ranges for Depression, Pain and Other Treatments
Safety: What the Data Shows
Patient sentiment around at-home safety is more cautious than the marketing of telehealth providers suggests. Of the patients we surveyed about at-home ketamine, 64.8% described it as “a bad idea.” The objection was usually framed in terms of monitoring during the dissociative state, not the medication itself.
That instinct is not unfounded. Ketamine produces dose-dependent dissociation, and a small subset of patients experience intense psychological reactions. In an in-clinic setting, vitals are monitored and a clinician can intervene immediately. At home, the patient is responsible for their own environment, and clinical response is delayed by whatever it takes to reach a phone or video call.
The medication itself is well tolerated. Fatalities from therapeutic ketamine doses are rare. The risk profile is dominated by setting and dose escalation, not the drug.
Access: Why At-Home Exists
Access is the strongest pro-telehealth argument, and patients agree. In our dataset, 58.1% said telehealth ketamine increases access to treatment. More tellingly, 44.9% cited access as their single biggest barrier to seeking ketamine therapy in any form.
HealingMaps maps 1,800 verified ketamine clinics across the United States. Coverage is concentrated in metro areas. A patient in rural Montana, west Texas, or northern Maine may sit 60 or more minutes from the nearest in-person provider. For those patients, the choice is not “at-home or in-clinic.” It is “at-home or no treatment.”
Scheduling is the secondary access lever. In-clinic protocols compress six sessions into two to three weeks, which is hard for shift workers, caregivers, and anyone without flexible PTO. At-home maintenance flexes around a normal week.
The Hybrid Model: How Most Clinics Now Operate
The cleanest finding from our 658-practitioner survey is that the binary “at-home versus in-clinic” framing is increasingly obsolete. Most established clinics now offer a hybrid pathway: an in-clinic induction series under direct supervision, followed by at-home maintenance with prescribed lozenges or rapid-dissolve tablets and continued clinician check-ins.
The hybrid approach captures the safety advantages of in-clinic care during the highest-risk window — first dose, dose titration, and the period when the patient is still learning their response — and shifts to a more affordable and flexible model once stability is established.
For patients evaluating providers, the right question is no longer “do you offer at-home or in-clinic?” The right question is “what is your protocol for stepping me from supervised to home administration, and how do you monitor maintenance?”
Routes of Administration
In-clinic IV: A 40-minute infusion at a controlled rate. Onset is rapid, dose precision is the highest of any route, and the clinician can pause or slow the infusion if the patient struggles.
In-clinic IM: A single intramuscular injection delivers the full dose. Onset is slightly slower than IV but still rapid. Once injected, the dose cannot be adjusted, so most clinics start IM patients at conservative doses.
At-home sublingual or rapid-dissolve: A lozenge or tablet held under the tongue or against the cheek. Onset is gradual (15–45 minutes), bioavailability is lower than IV or IM, and dose absorption varies between patients. The slower onset means a milder, longer experience — which some patients prefer and others find under-effective.
At-home intranasal: A nasal spray formulation. Onset and bioavailability fall between sublingual and IM. Less common in 2026 than sublingual at-home protocols.
Therapeutic Setting and Guidance
The setting question matters more than most patients expect. In a clinic, the room is built for the experience: dim lighting, a recliner, no interruptions, and a clinician within arm’s reach. At home, the patient builds the setting themselves. That can be more comfortable, or it can mean a roommate knocking on the door mid-session.
Guidance is similarly bifurcated. In-clinic providers often pair the dose with a therapist who is present during and after the session. At-home providers rely on virtual integration calls — useful, but a different experience than someone in the room.
WHY INTEGRATION MATTERS: First Data Showing Lack of Support During Psychedelic Integration May Lead to Harm
Who Should Pick Which
| Pick in-clinic if you… | Have severe treatment-resistant depression, are in active suicidal crisis, have a complex medical history, are starting ketamine therapy for the first time, or want IV titration for dose precision. |
| Pick at-home if you… | Have completed an induction series, are stable on maintenance, live more than 60 minutes from the nearest in-person clinic, or have inflexible scheduling and your provider has cleared you for home protocol. |
| Pick hybrid if you… | Want in-clinic safety during induction and at-home flexibility during maintenance. This is the model most established clinics now recommend by default. |
Firsthand Experiences
Beyond the decision framework, what these treatments actually feel like is part of the choice. Two HealingMaps editorial contributors share their experiences below.

At-Home Experience
One of our editorial contributors has done all of their ketamine experiences at home, using sublingual or intranasal administration prescribed by their physician and dispensed by compounding pharmacies. They found it useful, and it enhanced the therapy work they were already doing.
Their take: ketamine boosts neuroplasticity, but it does not do the work for you. Healthy habits, attention to thought and behavior patterns, and ongoing self-care are what convert a session into long-term change. The medicine is a window — what you do with it is the integration.
Some of their journeys went deep — occasionally frightening states of consciousness. In those moments, the absence of an in-person therapist or physician felt notable. They could imagine that having someone in the room would have helped them sit with the difficult parts and consider dose adjustments without anxiety.

In-Clinic IM and IV Experience
Our editor has had two deep experiences with medical professionals. He used 100 mg intramuscular, with an EMT, nurse, or doctor nearby. The big doses vaporized his regular world. He vanished into a strange dark realm, floating on a sea of nothingness.
The darkness felt blissful one second. The next minute he was dropping deeper into a hole, scared he was going to die.
With medical professionals nearby, though, he was able to relax, go inward, and say, “Ok, I’m ready to die.” Once he let himself “die,” his thoughts stopped, and he felt like he was part of the fabric of the cosmos.
“Dying” was not fun, exactly. Of course, he did not die. But the next day, he felt more content and more able to make hard decisions. He cleaned out a closet of old books and notebooks he had been holding onto for years.
The presence of medical professionals helped him go deeper. The feeling of “dying” gave him a new perspective on life and helped him let go of the past. The next time he did a big dose, he was even more able to relax.
Frequently Asked Questions
Is at-home ketamine FDA approved?
No. The only FDA-approved ketamine derivative for depression is Spravato (esketamine), and it must be administered in a certified clinic under direct observation. At-home ketamine is prescribed off-label by licensed clinicians and dispensed by compounding pharmacies.
Is at-home ketamine cheaper than in-clinic?
Per session, yes. Sublingual maintenance runs $150–250 per month. In-clinic IV or IM runs $300–500 per session. The total cost depends on protocol length — a six-session in-clinic induction can run $1,800–3,000 upfront, while at-home subscriptions are flat monthly.
Will my insurance cover either?
Probably not. In our 23,496-inquiry dataset, 75% of patients had zero insurance coverage for ketamine therapy. Spravato is the exception — when prescribed in-clinic, insured patients typically pay a $0–250 copay per session.
Can I switch from at-home to in-clinic, or vice versa?
Yes. Most clinicians will adjust your protocol based on response. Switching from at-home to in-clinic is common when patients want a deeper experience or are not progressing. Switching from in-clinic to at-home is common during maintenance, after the induction series.
Is at-home ketamine safe?
For appropriate patients, yes. The medication is well tolerated at therapeutic doses. The risk profile is dominated by setting and dose, not the drug. Patients with severe treatment-resistant depression, active suicidality, complex medical history, or no prior ketamine experience are generally better served by an in-clinic induction first.
The Bottom Line
The data is consistent: patients want both the safety of in-clinic care and the access of at-home care. The hybrid model — in-clinic induction stepping down to at-home maintenance — is how most established clinics now resolve the tension.
If you are starting ketamine therapy, default to in-clinic for the induction series. Use HealingMaps to find a verified clinic that offers a clear step-down protocol to at-home maintenance.
Find a verified ketamine clinic near you: Browse 1,800 mapped ketamine clinics across all 50 states.
READ NEXT: New To Ketamine Treatment? A Glossary of Ketamine Therapy Terms

