
What Are Psychedelics? We Explain The Differences From Other Drugs
Last reviewed and updated: May 11, 2026.
“Psychedelics” is a popular umbrella term that bundles three different drug classes with different mechanisms, different effects, and different legal status.
The word “psychedelic” was coined in 1956 by psychiatrist Humphry Osmond from Greek roots meaning “mind-manifesting.” In popular use it is shorthand for any drug that produces altered states of consciousness. Clinically, the category is more specific — and more divided — than the popular usage suggests.
This guide walks through the three psychedelic drug classes, the key compounds in each, what each produces, and where each stands legally and clinically in 2026.
Each class works on different brain receptors, produces a different experience, and sits in a different legal position. The side-by-side below covers all three.
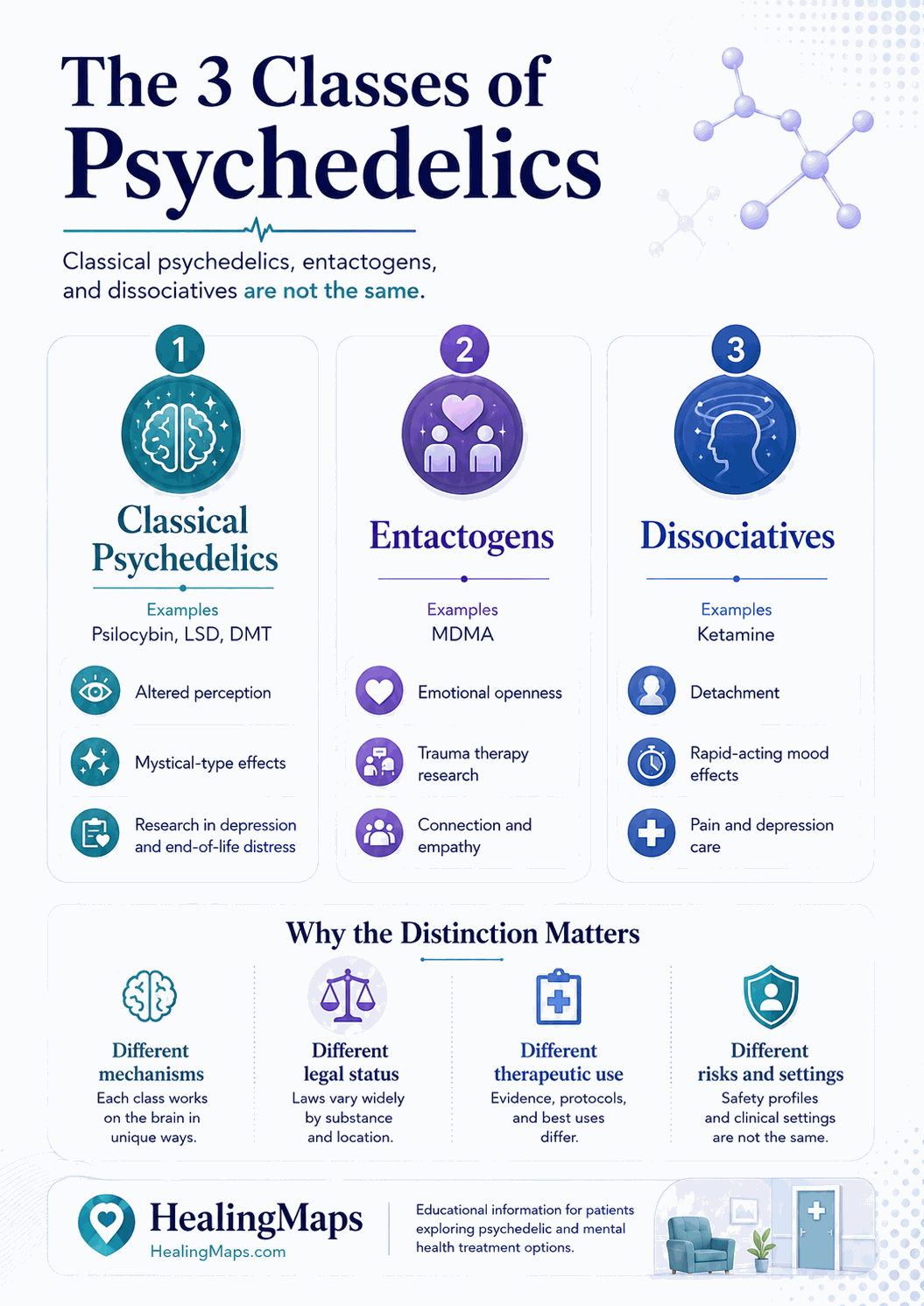
Class 1: Classical Psychedelics
Classical psychedelics work primarily through the serotonin 5-HT2A receptor. The class includes psilocybin (the active compound in magic mushrooms), LSD, DMT (the active compound in ayahuasca), and mescaline (in peyote and San Pedro cacti).
The experience is characterized by visual changes (geometric patterns, intensified colors, sometimes complex imagery), profound shifts in perception of time and self, and what users often describe as mystical or insight-driven states. Sessions typically last 4–8 hours depending on the compound.
Legal status (U.S., 2026): Federally Schedule I. Psilocybin specifically is legal in Oregon (Measure 109) and Colorado (Proposition 122) state programs through licensed service centers. Several cities have decriminalized possession (Denver, Oakland, Santa Cruz, Seattle, Detroit, Washington DC, others).
Clinical evidence: Psilocybin has shown efficacy in trials for treatment-resistant depression, alcohol use disorder, and end-of-life distress in cancer patients. Research is ongoing at Johns Hopkins, NYU, UCSF, and other institutions.
Class 2: Entactogens
Entactogens — sometimes called empathogens — work by triggering the release of serotonin and oxytocin. The defining compound is MDMA (3,4-methylenedioxymethamphetamine), commonly called ecstasy or molly in recreational contexts.
The experience is characterized by emotional openness, social warmth, reduced fear response, and a sense of connection. Visual and perceptual changes are minimal compared to classical psychedelics. Sessions typically last 4–6 hours.
Legal status (U.S., 2026): Federally Schedule I. MDMA-assisted therapy is in late-stage FDA review for PTSD treatment as of mid-2026. If approved, MDMA would become the first member of this class with regulated medical access.
Clinical evidence: Phase 3 trials of MDMA-assisted therapy for PTSD showed 67–71% remission rates in treated participants — among the strongest results documented for any PTSD intervention. Results published in Nature Medicine in 2021 and 2023.
Class 3: Dissociatives
Dissociatives work primarily by blocking the NMDA receptor, part of the brain’s glutamate signaling system. The clinical workhorse of this class is ketamine; related compounds include PCP and DXM.
The experience is characterized by dissociation from body and self — a sense of being separate from one’s physical experience, sometimes described as floating, sometimes as observing oneself from outside. Onset is faster and duration shorter than the other two classes (40–90 minutes for IV ketamine; up to several hours for at-home sublingual).
Legal status (U.S., 2026): Schedule III. Legal for prescription. Spravato (esketamine, a derivative) is FDA-approved for treatment-resistant depression and major depressive disorder with suicidality. Off-label use of generic ketamine for depression, PTSD, anxiety, and chronic pain is widespread.
Clinical evidence: The most extensive of the three classes, in part because ketamine has been clinically available the longest. Strong evidence for treatment-resistant depression, growing evidence for PTSD and chronic neuropathic pain.
What’s the Same Across All Three
All three classes can produce neuroplasticity — a temporary increase in the brain’s ability to form new connections and modify existing ones. This is one mechanism researchers think contributes to the durable effects of psychedelic therapy: the medication opens a window during which therapeutic insight, behavior change, and emotional processing become more possible.
All three are typically administered with structured therapeutic support. Set, setting, and integration matter as much as dose. The medication is not the treatment; the medication plus therapy plus integration is the treatment.
What’s Different
The differences come down to mechanism (serotonin vs. serotonin-release vs. glutamate), experience profile (perceptual vs. emotional vs. dissociative), duration (long vs. medium vs. short), and legal access.
For patients today, the legal-access difference is decisive. Ketamine is the only psychedelic regularly accessible nationwide outside of clinical trials and state pilot programs. That is why our 23,496-inquiry dataset is so heavily ketamine-weighted: it is the door most patients can actually walk through.
Common Misconceptions
“Ketamine is not a real psychedelic”
Some commentators argue ketamine should not be in the psychedelic category because it works through a different receptor system. Most clinical and research literature treats it as a dissociative subtype of psychedelic. The common element is profound alteration of consciousness with therapeutic potential.
“Microdosing makes psychedelics safe to use casually”
Sub-perceptual dosing reduces but does not eliminate risk. Sourcing remains unregulated in most jurisdictions. Recent placebo-controlled studies suggest expectancy effects account for a meaningful share of self-reported microdosing benefit.
“All psychedelics are illegal”
Ketamine has been a prescription medication since 1970. Spravato has been FDA-approved for depression since 2019. The “psychedelics are illegal” framing reflects classical psychedelics, not the full category.
Where Patients Actually Access Psychedelic Medicine in 2026
- Ketamine therapy — legal nationwide. 1,800 verified clinics in our directory.
- Psilocybin in Oregon — through licensed service centers under Measure 109.
- Psilocybin in Colorado — under Proposition 122, with regulated programs rolling out through 2026.
- Spravato (esketamine) — at REMS-certified clinics nationwide; generally insured.
- Clinical trials — psilocybin and MDMA studies recruiting through clinicaltrials.gov.
The Bottom Line
“Psychedelics” is a category, not a single substance. The three classes — classical, entactogens, dissociatives — work differently, feel different, and stand in different legal positions. For patients today, ketamine is the entry point: legal, accessible, and supported by the deepest clinical evidence base.
Find a verified ketamine clinic near you: Browse 1,473 mapped ketamine clinics across all 50 states.
READ NEXT: At-Home vs In-Clinic Ketamine: 2026 Cost, Safety & Access Data

