
The Clock Is Running on Ketamine Telehealth. Six Months Remain, and Many Clinics Are Not Ready
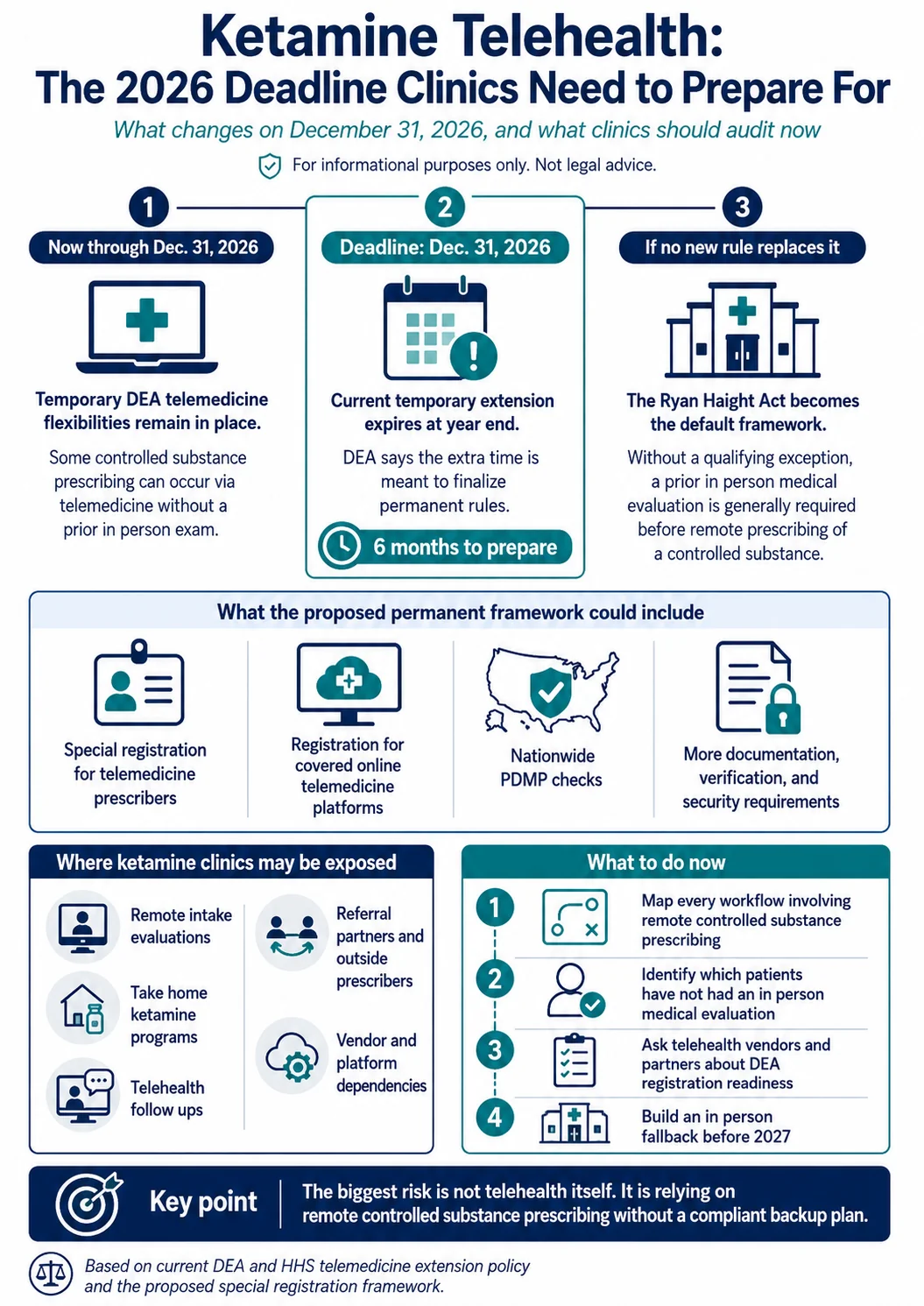
Every telehealth ketamine prescription written for a patient who has never been examined in person depends on a temporary rule. That rule expires December 31, 2026. The DEA has extended its pandemic era telemedicine flexibilities four times, and the agency has made clear this extension exists to finish permanent regulations, not to delay them.
The permanent framework on the table would reshape far more than the telehealth only companies everyone thinks of first. It reaches into referral relationships, prescribing platforms, and take home programs wherever controlled substance prescriptions are written remotely without a prior in person medical evaluation. Six months is enough time to prepare. It is not enough time to wait.
Preparing for the December deadline costs money. The Healing Health Alliance can help. HealingMaps’ GPO, the first built for the ketamine industry, gets member clinics 40 percent or more off medical supplies, 15 to 20 percent off malpractice and liability premiums, discounted LegitScript certification, and 20 to 30 percent off HIPAA compliant payment processing. Joining is free with no obligation. See what your clinic qualifies for →
Here’s An Overview
| Key Takeaway | Detail |
|---|---|
| The deadline is December 31, 2026 | The fourth extension of DEA telehealth flexibilities expires at year end |
| The default rule is strict | Without new rules, the Ryan Haight Act generally requires an in person exam before a remote controlled substance prescription, with narrow exceptions |
| Covered platforms would need DEA registration | The proposed framework would require covered online telemedicine platforms to register, not just prescribers |
| Nationwide PDMP checks are proposed | Prescribers would start with state level checks and eventually need to check every state and territory that maintains a PDMP |
| The stakes are real | The DEA’s own analysis estimates hundreds of thousands of first time telemedicine visits each year end in a controlled substance prescription |
| Past lapses hurt fast | When Medicare telehealth flexibilities lapsed during the October 2025 government shutdown, visits dropped 24 percent in 17 days |
Looking for treatment? Find Spravato clinics (which is covered by insurance) and ketamine clinics closest to you as well as other psychedelic therapies in your area.
Why This Deadline Is Different
The ketamine industry has lived through extension cycles before. Each time the deadline approached, the DEA extended. That pattern breeds complacency, and complacency is the risk.
This extension came with unusually direct language. The agencies stated the additional year exists to finalize permanent regulations, including the proposed Special Registration for Telemedicine. The DEA spent 2023 collecting more than 38,000 public comments on earlier proposals. Its January 2025 special registration framework drew another 6,475. The agency has signaled that requirements around registration, recordkeeping, and security are coming. The question is not whether the rules change. It is what the permanent framework demands.
What Happens if Nothing Replaces the Flexibilities
The fallback is the Ryan Haight Act of 2008. That law generally requires at least one in person medical evaluation before a practitioner can prescribe controlled substances remotely. Ketamine is a Schedule III controlled substance. Without a qualifying exception, no prior in person evaluation means no remote prescription.
The scale of disruption would be significant. In the economic analysis behind its proposed registration framework, the DEA estimated that hundreds of thousands of first time telemedicine visits each year result in a controlled substance prescription. And recent history shows how fast access collapses when telehealth rules lapse. When Medicare telehealth flexibilities lapsed during the October 2025 government shutdown, fee for service telemedicine visits dropped 24 percent nationally in the first 17 days. Some states saw declines at or above 40 percent.
The Platform Registration Rule Nobody Is Discussing
Most coverage of the special registration proposal focuses on prescribers. The provision with the widest reach sits elsewhere. The proposed framework would require covered online telemedicine platforms, meaning companies that facilitate connections between patients and prescribers for care that can end in a controlled substance prescription, to register with the DEA themselves. Not every scheduling tool or video vendor would qualify as covered. Any platform built around connecting patients to prescribers should assume it might.
Think through what that touches. Any clinic that uses a third party telehealth vendor for intakes or follow ups now has a compliance dependency it does not control. Any referral relationship with a telehealth ketamine company depends on that company securing and keeping a DEA registration. Platform registration turns your technology stack into a regulatory question. Ask your vendors now whether they are preparing to register. Their answer tells you whether your workflow survives 2027 intact.
What Else Sits Inside the Proposed Framework
The special registration proposal creates tiered pathways. A standard registration would cover Schedule III through V prescribing via telemedicine, which includes ketamine. An advanced tier would cover Schedule II drugs and would be limited to specific board certified specialists, including psychiatrists.
The proposal also moves toward nationwide prescription database checks. Prescribers would initially check the PDMPs of the states where they and the patient are located, plus reciprocal states. Three years in, they would need to run comprehensive checks across every state and territory that maintains a PDMP before writing a script. For ketamine prescribers, that means diversion red flags become visible, and so does your own prescribing pattern. The DEA also sought comment on additional safeguards, including requiring prescribers to be located in the same state as the patient for Schedule II drugs. Requirements like these signal the agency’s direction: more verification, more documentation, more visibility.
Why Brick and Mortar Clinics Cannot Sit This Out
Infusion clinics often treat the telehealth cliff as someone else’s problem. Look closer at your own operation before settling into that view.
Does your clinic conduct initial evaluations by video? Does your medical director prescribe sublingual ketamine for maintenance between infusion series? Do you refer patients to a telehealth partner when they move away or cannot travel? Each of those touchpoints runs through the expiring flexibilities. The dividing line is not telehealth versus in person care. It is whether a controlled substance prescription is written without a prior in person evaluation. State rules like the ones Texas proposed this year govern what happens inside your treatment rooms. The federal rules govern the remote layer, and nearly every modern practice has one.
What to Do With the Six Months
Start with an audit. List every workflow where a controlled substance prescription happens without a prior in person visit. Intakes, refills, maintenance protocols, referral handoffs. That list is your exposure.
Then build the in person fallback. Practices that can convert remote first patients to at least one in person evaluation hold the strongest position no matter what the final rule says. An initial in person visit satisfies the Ryan Haight Act permanently for that patient relationship.
Finally, watch the rulemaking. The DEA said permanent regulations will arrive before the December deadline. When the final rule publishes, the transition window will be short. Clinics that mapped their dependencies in July will adapt in weeks. Clinics that ignored the deadline will face January with a broken intake funnel.
The ketamine industry got a one year reprieve. Half of it is already gone.

