Semaglutide vs. Tirzepatide: Complete 2026 Comparison
Last reviewed and updated: May 5, 2026 — medically reviewed by Dr. Jonathann Kuo, MD.
2026 Update: In the SURMOUNT-5 head-to-head trial, tirzepatide produced ~47% more weight loss than semaglutide over 72 weeks. Both medications remain FDA-approved and widely prescribed, with compounded versions increasingly available through licensed 503A and 503B pharmacies.
Whichever molecule wins for you, the cheapest GLP-1 online guide shows who prescribes it for the least.
Semaglutide and tirzepatide are the two most-prescribed peptide medications in the United States. Both are GLP-1-based, once-weekly injections approved for weight management and type 2 diabetes. They sit at the center of a $100 billion-plus market projected by the end of the decade. If you are deciding between them — or trying to understand the difference between Wegovy, Ozempic, Zepbound and Mounjaro — this guide walks through what the clinical evidence actually shows.
Looking for a clinic? Find verified GLP-1 and peptide therapy clinics near you.
The Short Answer
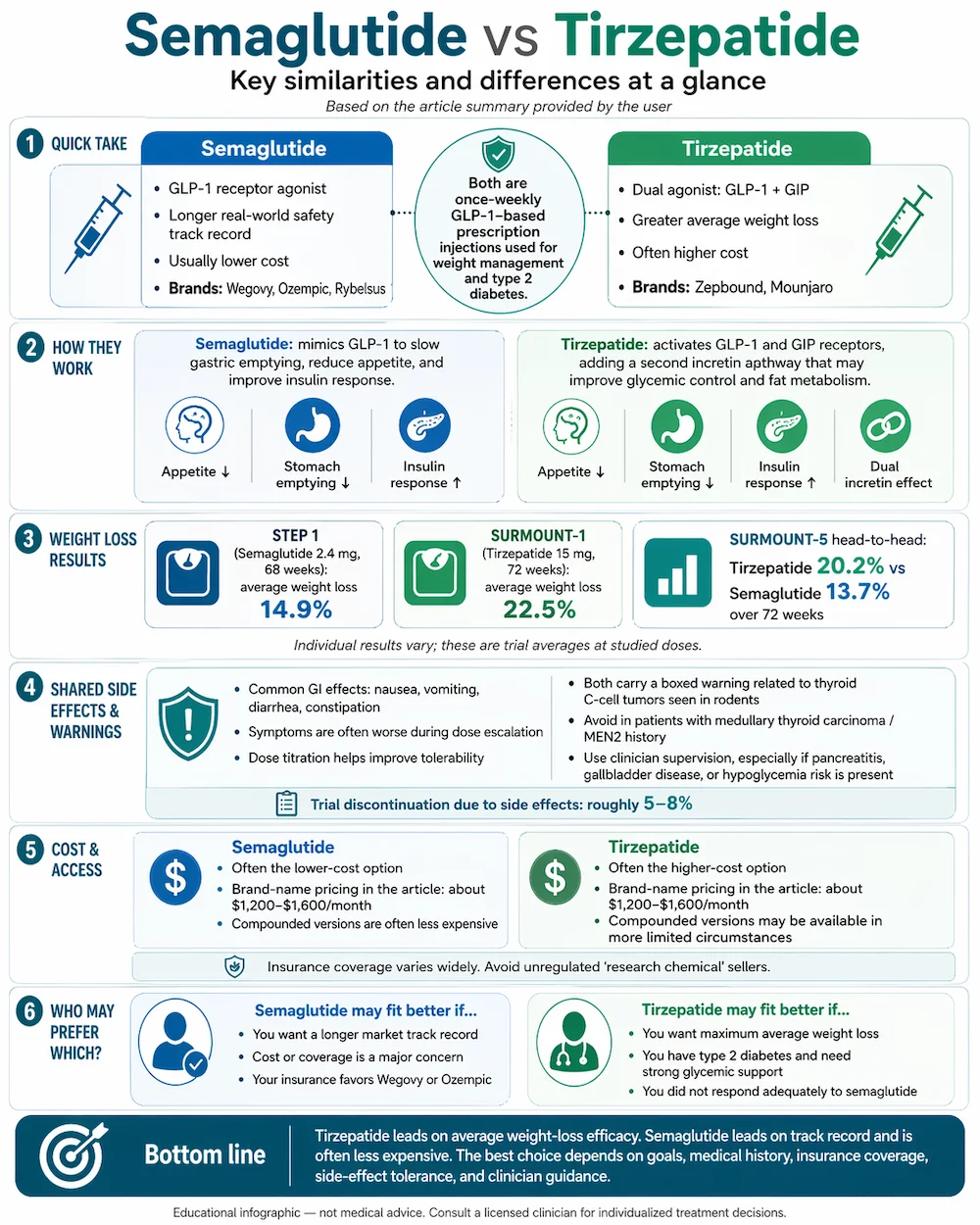
Tirzepatide produces more weight loss on average. Semaglutide has the longer real-world safety track record and typically costs less. Both work through related but distinct mechanisms, both are administered as once-weekly subcutaneous injections, and both require a licensed clinician to prescribe. The right choice depends on specific goals, medical history, insurance coverage and cost tolerance — a decision best made with a qualified provider.
Doctor-prescribed GLP-1s — delivered to your home
Get doctor-prescribed GLP-1s shipped straight to your door — no insurance needed, from $199/mo.
SkinnyRx pairs prescription GLP-1 medication with clinician-guided care: compounded semaglutide from $199/mo, or tirzepatide from $299/mo as a once-weekly injection or once-daily tablet. Online assessment, licensed provider review, free shipping, cancel anytime — FSA/HSA eligible.
Check If I Qualify →Provider consultation required. HealingMaps may earn a commission through this link — it doesn’t change your price. Compounded medications are not FDA-approved finished products; eligibility is determined by SkinnyRx’s licensed providers. 90-day money-back guarantee per SkinnyRx terms.
What Each Peptide Is
Semaglutide is a synthetic peptide that mimics glucagon-like peptide-1 (GLP-1), a natural incretin hormone released in the gut after eating. By binding GLP-1 receptors, it slows gastric emptying, reduces appetite and improves insulin sensitivity. It is FDA-approved under three brand names: Wegovy (for weight loss), Ozempic (for type 2 diabetes) and Rybelsus (an oral form for diabetes). All three contain the same molecule at different doses and formulations.
Tirzepatide is a newer synthetic peptide that binds two incretin receptors at once: GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). This dual mechanism is why tirzepatide is sometimes described as a “twincretin.” It is FDA-approved under two brand names: Zepbound (for weight loss) and Mounjaro (for type 2 diabetes). For a broader look at how these compounds fit into the peptide landscape, read our GLP-1 overview.
Weight Loss Efficacy: What the Trials Show
The most reliable data comes from the manufacturers’ pivotal trials, which are large, randomized, placebo-controlled and FDA-reviewed.
STEP 1 — Semaglutide
The landmark semaglutide trial, published in the New England Journal of Medicine in 2021, randomized 1,961 adults with obesity to semaglutide 2.4 mg weekly or placebo for 68 weeks. The semaglutide group lost an average of 14.9% of body weight compared to 2.4% in the placebo group. About 86% of the semaglutide group achieved at least 5% weight loss. Subsequent STEP trials (2 through 8) have replicated the effect across different populations and dosing schedules.
SURMOUNT-1 — Tirzepatide
The pivotal tirzepatide trial, published in the New England Journal of Medicine in 2022, randomized 2,539 adults with obesity to tirzepatide 5 mg, 10 mg, 15 mg or placebo for 72 weeks. At the highest dose, participants lost an average of 22.5% of body weight. At the 15 mg dose, 91% achieved at least 5% weight loss and 57% achieved at least 20%. These figures are dose-dependent — lower doses produce less weight loss.
SURMOUNT-5 — Head-to-Head
In 2025, Eli Lilly published the SURMOUNT-5 trial directly comparing tirzepatide (15 mg) and semaglutide (2.4 mg) in adults with obesity over 72 weeks. Tirzepatide produced approximately 20.2% weight loss versus 13.7% for semaglutide — about 47% more weight loss on an absolute basis. This head-to-head data settled the efficacy question: on average, tirzepatide out-performs semaglutide for weight loss at maximum doses.
Two caveats are important. First, these are averages — individual response varies widely, and some patients respond better to semaglutide for reasons that are not yet fully understood. Second, “more weight loss” is not automatically “better” for every patient; tolerance, comorbidities and cost all factor in.
Mechanism of Action
Semaglutide acts on a single receptor: GLP-1. When activated, GLP-1 receptors trigger a cascade that slows stomach emptying, lengthens the time food takes to leave the gut, boosts insulin release in response to glucose, and reduces appetite signals in the hypothalamus. The net effect is that patients feel full sooner, stay full longer and eat less.
Tirzepatide adds a second mechanism on top of the same GLP-1 effects. GIP is another incretin hormone released by the gut. Alone, GIP has a relatively modest effect on appetite and weight. Combined with GLP-1 agonism, however, it amplifies insulin secretion and appears to improve fat metabolism in ways that exceed GLP-1 alone. This synergy is the theoretical basis for tirzepatide’s superior weight loss in head-to-head trials.
Side Effects and Tolerability
The side-effect profiles are remarkably similar. Both medications most commonly produce gastrointestinal symptoms: nausea, vomiting, diarrhea and constipation. Most symptoms occur during dose escalation and tend to subside as the body adapts. Roughly 5 to 8% of patients in clinical trials discontinued due to side effects. Dose titration — starting low and increasing gradually — substantially reduces side effect severity.
Both medications carry a boxed warning about thyroid C-cell tumors observed in rodent studies (though not confirmed in humans) and are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2. Pancreatitis, gallbladder disease and hypoglycemia (when combined with insulin or sulfonylureas) are additional considerations. These medications should always be prescribed and monitored by a licensed clinician.
Cost and Access
Brand-name list pricing in 2026 runs roughly $1,200 to $1,600 per month for Zepbound or Wegovy without insurance. The manufacturers now sell direct to cash-pay patients for far less: Zepbound runs $299 to $449 per month through LillyDirect by dose, and Wegovy runs $349 per month for standard doses through NovoCare Pharmacy ($199 per month on the first two fills through December 2026). Ozempic and Mounjaro (the diabetes-indicated brands) can sometimes be obtained at lower prices when prescribed for diabetes. Insurance coverage varies widely — some plans cover these medications for obesity, many do not.
Compounded versions — typically produced by 503A or 503B licensed pharmacies — have emerged as a lower-cost pathway. Monthly prices for compounded semaglutide typically run $200 to $400; compounded tirzepatide runs $250 to $500. The FDA removed tirzepatide from its drug shortage list in late 2024, which changed the legal landscape for compounding. As of 2026, compounded versions are legally available in more limited circumstances; patients should confirm with their clinician and pharmacy that the sourcing is compliant.
Important: Avoid unregulated online vendors marketing semaglutide or tirzepatide as “research chemicals.” These products are not tested for human use and have been found in independent testing to vary dramatically in purity and concentration.
Who Should Choose Which?
This is always a clinical decision, but some patterns have emerged in the way providers describe their prescribing preferences:
- Tirzepatide tends to be preferred for patients seeking maximum weight loss, patients with type 2 diabetes (where the dual mechanism helps glycemic control), and patients who have not responded adequately to semaglutide.
- Semaglutide tends to be preferred for patients prioritizing the lower-cost option, patients who want the longer real-world safety track record (semaglutide has been on the market longer), and patients with insurance coverage that favors Wegovy or Ozempic.
- Neither is preferred for patients with a history of thyroid cancer, severe gastroparesis or a personal/family history of medullary thyroid carcinoma.
Brand vs Compounded Considerations
Branded and compounded versions of these peptides are not equivalent in every regulatory sense. Branded Wegovy, Ozempic, Zepbound and Mounjaro are FDA-approved finished drug products manufactured to strict pharmacopeial standards. Compounded versions are prepared by licensed compounding pharmacies under state-level regulation, with oversight from the FDA’s 503A or 503B pathway.
Compounded versions often include additives like vitamin B6 or other peptides, and dosing may differ from the branded equivalents. For patients using compounded versions, the critical questions to ask a clinic are: is the compounding pharmacy 503A or 503B registered? Does it test for purity, sterility and concentration? Is third-party lab testing available? The answers matter for both safety and efficacy.
Doctor-prescribed GLP-1s — delivered to your home
Get doctor-prescribed GLP-1s shipped straight to your door — no insurance needed, from $199/mo.
SkinnyRx pairs prescription GLP-1 medication with clinician-guided care: compounded semaglutide from $199/mo, or tirzepatide from $299/mo as a once-weekly injection or once-daily tablet. Online assessment, licensed provider review, free shipping, cancel anytime — FSA/HSA eligible.
Check If I Qualify →Provider consultation required. HealingMaps may earn a commission through this link — it doesn’t change your price. Compounded medications are not FDA-approved finished products; eligibility is determined by SkinnyRx’s licensed providers. 90-day money-back guarantee per SkinnyRx terms.
Frequently Asked Questions
Is tirzepatide always better than semaglutide?
On average, tirzepatide produces more weight loss at maximum dose. That does not make it the right choice for everyone. Individual response varies, cost matters, and tolerance to GI side effects during dose escalation differs. Many patients do well on semaglutide and never need to try tirzepatide.
Can I switch from one to the other?
Yes, many clinicians transition patients between the two when weight loss plateaus, side effects become intolerable or supply issues arise. The switch is not a simple 1:1 conversion — dosing typically restarts at a lower level to reduce side effects, then titrates up. Any transition should be clinician-directed.
What happens when I stop taking semaglutide or tirzepatide?
Weight regain is common. The STEP 1 extension data showed that patients who stopped semaglutide regained about two-thirds of the weight they had lost within a year. This is why both medications are generally considered long-term therapies rather than short-term interventions. Lifestyle changes (diet, exercise, sleep) improve weight maintenance, but do not fully prevent regain in most patients.
Are there other next-generation GLP-1 peptides coming?
Yes. Retatrutide, a triple-agonist (GLP-1, GIP and glucagon), is in late-stage trials and has produced even more weight loss in early data — up to 24% at 48 weeks in phase 2. It is not yet FDA-approved. Several other dual and triple agonists are in the pipeline.
Can I take BPC-157 or other peptides alongside semaglutide or tirzepatide?
Many clinics do stack GLP-1 medications with other peptides — for example, pairing tirzepatide with BPC-157 for patients who experience joint pain as they lose weight, or with CJC-1295 and Ipamorelin for muscle preservation. These combinations require clinician oversight and are not studied in formal clinical trials.
The Bottom Line
Tirzepatide wins on weight-loss efficacy in head-to-head trials. Semaglutide wins on cost and real-world track record. Both are legitimate, FDA-approved options and both require a licensed clinician, proper medical evaluation and ongoing monitoring. For most patients, the “best” choice is less about which molecule is theoretically superior and more about which one is accessible, affordable and tolerated — answers that depend on individual circumstances a provider can help work through.
Ready to talk to a clinician? Browse our directory of verified peptide therapy clinics to find a licensed provider near you.
- What Is Peptide Therapy? Complete 2026 Guide
- GLP-1: The Next Frontier of Peptide Wellness
- Retatrutide: The Trillion-Dollar Weight-Loss Peptide
- FDA Peptide Reclassification: What the 2026 Changes Mean
Ready to compare actual providers? We’ve vetted four GLP-1 telehealth programs on price, refund policies, and pharmacy quality — see our 2026 GLP-1 telehealth programs comparison for the side-by-side.