Sermorelin vs. CJC-1295 vs. Ipamorelin: The 2026 Growth Hormone Peptide Guide
Last reviewed and updated: May 5, 2026 — medically reviewed by Dr. Jonathann Kuo, MD.
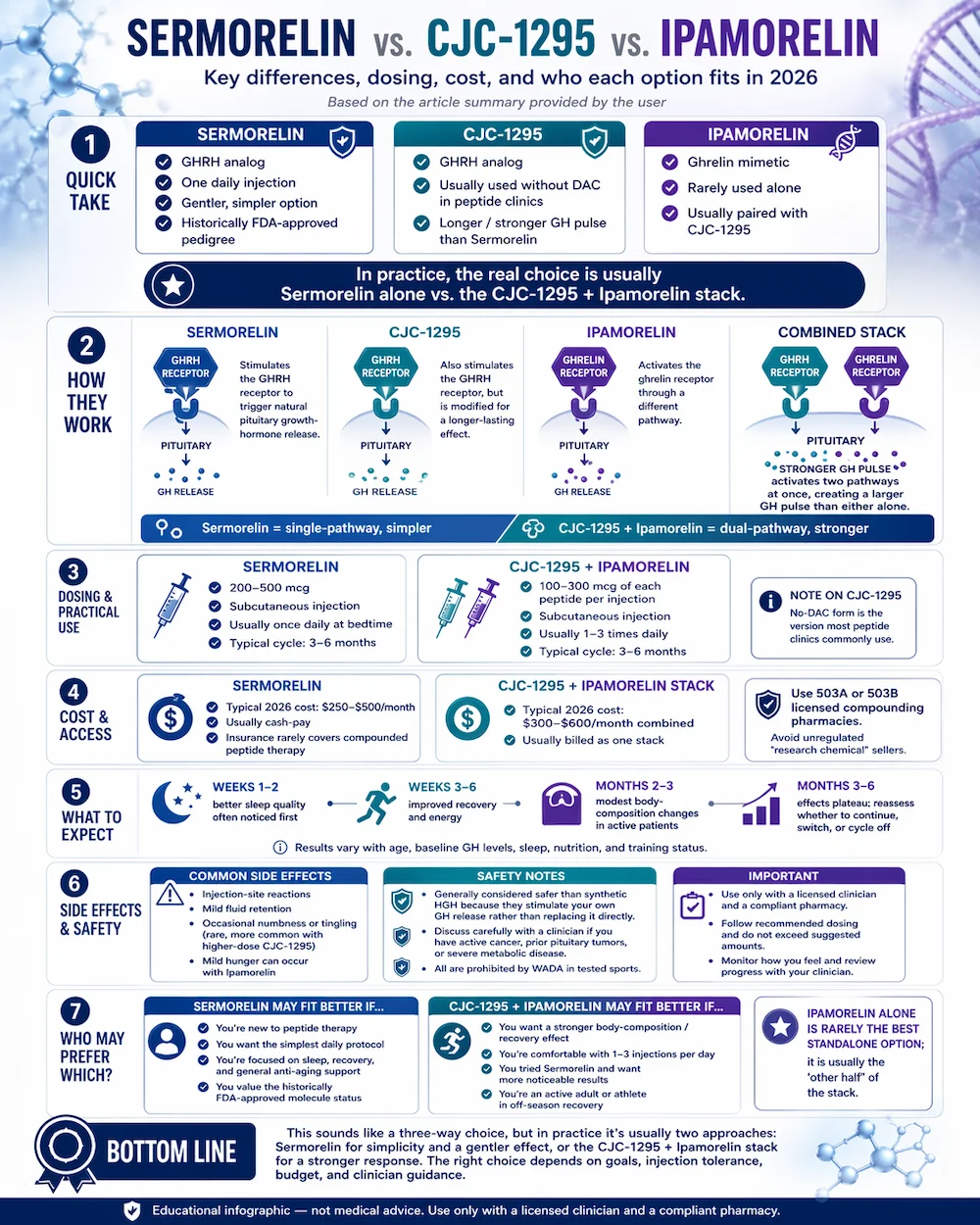
The Short Version: There are really only two choices here. Sermorelin is the gentler, one-injection-a-day option with a historical FDA-approved pedigree. CJC-1295 and Ipamorelin are almost always prescribed together as a stronger stack — neither is typically used alone. This guide walks through which option fits which patient.
Three growth-hormone peptides dominate the market today: Sermorelin, CJC-1295, and Ipamorelin. Patients ask about all three because they all show up in clinic websites, forums and YouTube videos — often without explaining how they actually relate to each other. The real decision is simpler than the menu suggests. Let’s walk through what each one does, how they’re prescribed, and which option fits which kind of patient.
Looking for a clinic? Find verified growth-hormone peptide clinics near you.
The Short Answer
If you are choosing between growth-hormone peptides in 2026, your real decision is between two approaches. Sermorelin alone is the simpler, gentler option — one injection a day, historically FDA-approved as a drug product, and closest to how your body naturally releases growth hormone. CJC-1295 stacked with Ipamorelin is the stronger, more popular modern option — two peptides injected together 1 to 3 times daily, producing a bigger growth-hormone pulse than either molecule alone. Ipamorelin is rarely prescribed by itself; it is almost always the “other half” of the CJC-1295 stack.
The single-peptide route
Prefer Sermorelin’s simplicity? Prescribed online from $119.
If once-daily Sermorelin fits you better than a multi-peptide stack, Strut Health prescribes it 100% online — quick intake, doctor review, and it ships to your door as an injection or needle-free lozenge.
Check If I Qualify →Physician consultation required; compounded and dispensed by licensed U.S. pharmacies. HealingMaps may earn a commission through this link — it doesn’t change your price. Compounded sermorelin is not an FDA-approved finished product; eligibility is determined by Strut’s physicians.
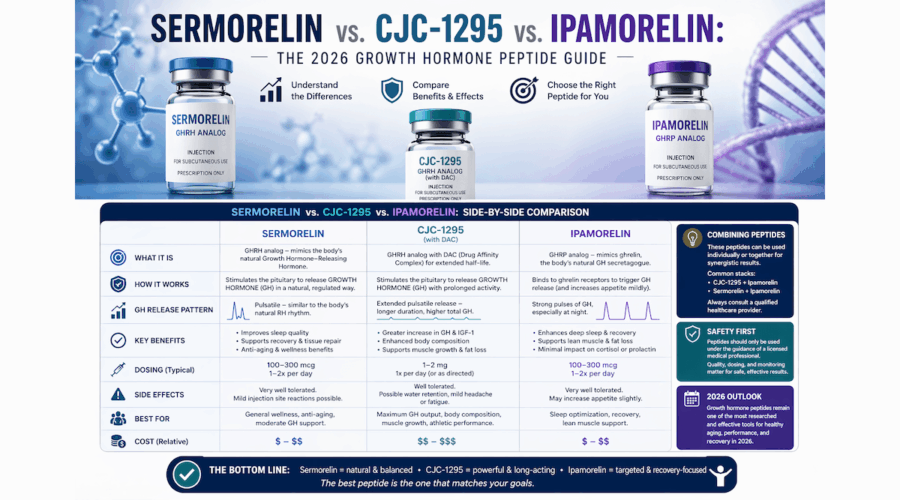
What Each Peptide Is
Sermorelin is a 29-amino-acid peptide that acts as a growth-hormone-releasing hormone (GHRH) analog. It binds the same pituitary receptor that the body’s own GHRH targets, telling the pituitary gland to release growth hormone in the same way it would naturally. Sermorelin was originally sold under the brand name Geref, which received FDA approval in the 1990s for pediatric growth hormone deficiency. That original branded product has been discontinued, but the molecule remains available through compounding pharmacies on a physician prescription.
CJC-1295 is a 30-amino-acid peptide. Like Sermorelin, it is a GHRH analog — it stimulates the same pituitary receptor. The difference is a modification to the molecule that extends how long it stays active in the body, giving a longer and more sustained growth-hormone pulse per injection. CJC-1295 comes in two forms: “with DAC” (long-acting, 8-day half-life) and “without DAC” (short-acting, also called Modified GRF 1-29). The no-DAC form is the one most peptide clinics use, and it is almost always paired with Ipamorelin.
Ipamorelin is a 5-amino-acid peptide and the shortest of the three. It is not a GHRH analog — it is a ghrelin mimetic, meaning it binds the ghrelin receptor (the same receptor activated by the “hunger hormone”). Activating that receptor triggers a pulse of growth hormone release through a different pathway than GHRH. Ipamorelin is described as “selective” because it doesn’t raise cortisol or prolactin the way earlier GHRP peptides did. On its own, Ipamorelin produces a modest growth-hormone effect. Combined with CJC-1295, the two mechanisms stack.
Why CJC-1295 and Ipamorelin Are Almost Always Prescribed Together
The pituitary has two distinct pathways for releasing growth hormone: the GHRH receptor and the ghrelin receptor. Activating just one produces a moderate growth-hormone pulse. Activating both at the same time produces a substantially larger pulse — more than the sum of the two individual effects. That’s the pharmacological case for stacking a GHRH analog (CJC-1295) with a ghrelin mimetic (Ipamorelin).
In practice, this means most peptide clinics prescribe CJC-1295 and Ipamorelin as a single combined injection or as two injections at the same time each day. The combined price is typically billed as one stack, and the dosing schedule is designed around the pair rather than either compound individually. If a patient asks for “just Ipamorelin,” most clinicians will recommend adding CJC-1295 to get meaningful results.
Sermorelin vs. the CJC + Ipamorelin Stack
Practically speaking, the choice most patients face is Sermorelin alone or the CJC + Ipamorelin stack. Each approach has genuine trade-offs.
Sermorelin wins on simplicity. One injection a day, typically at bedtime to match the natural growth-hormone release cycle. Historically FDA-approved molecule. Gentler effect closer to the body’s own rhythm. Most favored for patients new to peptide therapy, those optimizing for sleep and general recovery, and those who want the simplest daily protocol.
The CJC + Ipamorelin stack wins on effect size. The dual-receptor mechanism produces a larger growth-hormone pulse, which translates to more noticeable changes in body composition, recovery, and sleep depth. Most favored for active adults focused on body composition, athletes in the off-season, and patients who have tried Sermorelin and want a stronger response. The trade-off is 1 to 3 injections per day instead of one, and a slightly higher monthly cost.
Dosing and Administration
Sermorelin is administered via subcutaneous injection once daily, typically at bedtime. Standard doses run 200 to 500 micrograms per day. A typical cycle runs 3 to 6 months. Some clinicians continue indefinitely for anti-aging and sleep optimization under ongoing supervision.
CJC-1295 (no DAC) plus Ipamorelin is administered via subcutaneous injection 1 to 3 times per day, often as a single combined injection. Typical doses run 100 to 300 micrograms of each peptide per injection. Protocols vary — some clinicians dose once daily before bed; others use two or three injections spaced through the day to maximize the pulse pattern. Cycles typically run 3 to 6 months with off-cycles of similar length.
All three peptides should be sourced through 503A or 503B licensed compounding pharmacies. Products marketed as “research chemicals” online are not tested for human use and have been found in independent testing to vary dramatically in purity and concentration. Reputable clinics will name their pharmacy partner and share testing documentation on request.
Cost and Access
Typical 2026 US pricing through compounding pharmacies:
- Sermorelin alone: $250 to $500 per month, depending on dose and clinic model.
- CJC-1295 + Ipamorelin stack: $300 to $600 per month combined.
- Ipamorelin alone (rare): usually billed as part of the stack — standalone pricing is uncommon.
Insurance almost never covers compounded peptide therapy, so these are cash-pay figures. Clinics often bundle consultation fees, follow-up visits, and lab work into a monthly membership price — look carefully at what’s included before comparing quotes.
HealingMaps may earn a commission when readers sign up through Strut Health. This does not affect our editorial coverage or your price. Sermorelin is a prescription medication; eligibility is determined by a licensed clinician. Pricing reflects Strut Health’s published $99/month rate and may change.
For a deeper breakdown of what each protocol actually costs across clinic models — including the telehealth routes that undercut in-person pricing — see our complete Sermorelin cost guide.
What to Expect From a Cycle
Timeline is similar across all three peptides because they ultimately affect the same downstream hormone — your own endogenous growth hormone. Most patients report:
- Weeks 1 to 2: Better sleep quality is usually the first noticeable effect. Deeper, more restorative sleep.
- Weeks 3 to 6: Improved energy and recovery from workouts. Reduced joint soreness in patients who had it at baseline.
- Months 2 to 3: Visible changes in body composition — typically modest fat loss around the midsection and improved muscle tone in active patients. Libido and skin quality improvements reported in some patients.
- Months 3 to 6: Full effects plateau. This is the point where most clinicians evaluate whether to continue, switch approaches, or cycle off.
Individual response varies. Some patients see more dramatic effects; others see subtle improvements. Age, baseline growth-hormone levels, sleep quality, nutrition, and training status all affect outcomes.
Safety and Side Effects
All three peptides have favorable safety profiles. Because they stimulate the body’s own growth-hormone release rather than introducing exogenous growth hormone, they’re generally considered safer than synthetic HGH therapy. That said, real side effects exist:
- Injection-site reactions — redness, minor swelling, occasional bruising. Usually resolves within days.
- Mild fluid retention — some patients experience mild water retention, particularly in the first 2 to 4 weeks.
- Occasional numbness or tingling — rare, more common with CJC-1295 at higher doses.
- Mild hunger — occasionally reported with Ipamorelin due to slight ghrelin-receptor activity.
Patients with active cancer, a history of pituitary tumors, or severe metabolic disease should discuss growth-hormone peptide therapy carefully with both their primary clinician and specialist before starting. This is not universal contraindication territory, but it warrants careful evaluation.
Who Should Consider Which?
- Sermorelin alone — patients new to peptide therapy, those focused on sleep and general anti-aging, patients who prefer the simplest daily protocol, and those who value the historically FDA-approved molecule status.
- CJC-1295 + Ipamorelin stack — active adults focused on body composition, athletes in off-season recovery, patients who tried Sermorelin and want stronger effects, and those comfortable with 1 to 3 injections per day.
- Ipamorelin alone — rarely prescribed; when used alone it is typically for patients who need the ghrelin-pathway effect without a GHRH analog for a specific clinical reason.
Some clinicians move patients through a progression: start with Sermorelin to establish tolerability and baseline response; switch to the CJC + Ipamorelin stack if a stronger effect is desired. Others prescribe the stack from day one for patients specifically focused on body composition.
Frequently Asked Questions
Can I switch between Sermorelin and the CJC-1295 / Ipamorelin stack?
Yes. Many patients start with Sermorelin to establish response, then switch to the CJC + Ipamorelin stack for stronger effect. The transition does not require a washout period — most clinicians simply stop one and start the other. Any switch should be clinician-directed.
How are these different from synthetic HGH therapy?
Synthetic human growth hormone (somatropin) introduces exogenous growth hormone directly into the body. Sermorelin, CJC-1295 and Ipamorelin instead stimulate the pituitary to release the body’s own growth hormone in a more natural pulsatile pattern. The peptide approach is generally considered safer, because the body’s normal feedback loops remain intact — it’s harder to overshoot physiologic levels. Synthetic HGH is also significantly more expensive and requires stricter prescribing conditions.
Do these peptides cause weight loss?
They can contribute to modest body-composition changes, typically reducing visceral fat and improving muscle tone over 2 to 3 months of use. They are not weight-loss medications in the way semaglutide or tirzepatide are. Expect body-composition shifts over months, not dramatic weight loss.
Can I stack these with other peptides?
Yes, very commonly. Active adults often combine a growth-hormone peptide stack with BPC-157 and TB-500 for recovery, KPV for inflammation, or PT-141 for sexual wellness. Combinations should be clinician-directed.
Are these banned in sports?
Yes. All three peptides are prohibited by the World Anti-Doping Agency (WADA) because they increase endogenous growth hormone. Athletes subject to drug testing should consult a sports medicine physician familiar with WADA rules before considering any of these compounds.
How long can I stay on growth-hormone peptide therapy?
Most clinicians recommend cycles of 3 to 6 months on, followed by an off-cycle of equivalent length. This lets the body’s natural growth-hormone signaling reset between courses. Some patients run indefinite low-dose Sermorelin protocols under ongoing clinical supervision; the stack is more typically cycled.
The Bottom Line
The three growth-hormone peptides sound like a three-way choice, but in practice the decision is between two approaches. Sermorelin is the simpler, gentler option — one injection a day, closer to the body’s natural rhythm, historically FDA-approved pedigree. The CJC-1295 and Ipamorelin stack is the stronger modern option — more injections per day, larger growth-hormone pulse, more pronounced effects on body composition and recovery. Ipamorelin alone is rarely the right answer; it’s the “other half” of the stack rather than a standalone choice. Any of these protocols should be clinician-directed, with baseline labs, a compliant compounding pharmacy, and a clear plan for how you’ll evaluate response at the 3-month mark.
HealingMaps may earn a commission when readers sign up through Strut Health. This does not affect our editorial coverage or your price. Sermorelin is a prescription medication; eligibility is determined by a licensed clinician. Pricing reflects Strut Health’s published $99/month rate and may change.
Ready to find a clinic? Browse our directory of verified growth-hormone and recovery peptide clinics to find a licensed provider near you.

